It is likely that everyone has heard the importance of stretching, and how it can be of benefit in maintaining range of motion, improving function and preventing injury. This sounds like it would be the case for the Cerebral Palsy (CP) population- particularly as a main characteristic of CP is muscle hyper-resistance (high resistance to stretch) ; this is alongside reduced muscle length and increased joint stiffness….but apparently, this may not be the case.
A recent review by Kalkman et al (2020) suggests that there are little to no improvements on muscle function from stretching protocols used in children with CP.
But why is this the case?
Studies have shown that there are differences in the muscles and tendons of children with CP when compared to typically developing children. Including:
- Shorter muscle length and longer tendon lengths
- Shorter muscle fascicles (bundles of muscle fibres)
- Limited potential for active shortening
- Reduced force generation capacity
- Changes in muscle and tendon growth factors
Due to these changes, as well as changes in the joint stiffness and the way in which the musculotendinous unit (MTU) responds to stretching, it potentially may not be helpful in increasing muscle length or improving range of motion.
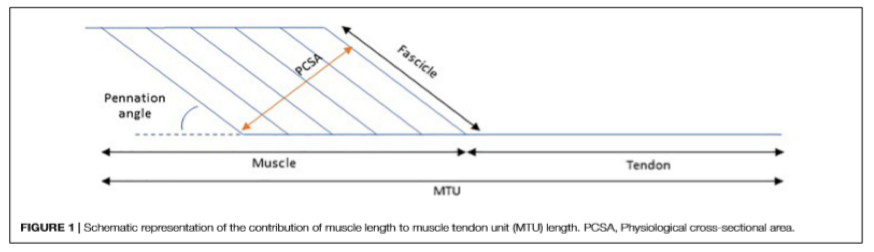
Kalkman et al (2020) propose that one reason that stretching (passive, serial casting or Ankle-foot orthoses) may be ineffective, is that the majority of these interventions do not sufficiently stimulate a stretch in the muscle- they primarily target the tendon part of the MTU (i.e. the tendon is what “sees” most of the stretch applied).
Imagine you are pulling at a cord tied to something. The part of the cord closest to you is made of elastic, and then the part tied up is made of rope. If you try and pull the rope away from what it is tied to, the elastic part of the cord is going to stretch out a lot easier and quicker than the rope part. This is similar to what is happening in the muscle-tendon unit in someone with CP- the tendon is the elastic, and the muscle is the rope….The tendon is the thing that is seeing the most of the stretch.
Although some interventions can improve range of motion of the whole MTU, changes in actual muscle length seems to have very minimal (if any) contribution to these changes. The tendon stretch, the impact of passive structures, and increased stretch tolerance seem to have the most influence on any changes seen in range of motion.
Perhaps these interventions are not able to achieve improvements in function, as they do not target the actual “muscle” part of the MTU well enough, which is the component that would potentially result in functional changes.
So what can we do to improve the effectiveness of stretching in CP populations? Some ideas from research
- Botulinum Toxin- A and stretching: Botox injections can reduce the amount of resistance in the muscle, which allows it to receive more of a stretch when it is applied.
- Electrical stimulation and stretching- Stimulating the muscle/s that does the opposite action of the one you are trying to stretch (i.e. stimulating the muscles that straighten the knee) can help to create a relaxation response in the muscle/s you want to stretch (I.e. the muscles that bend the knee). This means you may be able to achieve a greater stretch in the muscle.
- “Eccentric fascicle loading” (i.e.“active stretches”)- Loading of the muscle whilst it is in a lengthened position can help to increase the stretch. Methods such as backward downhill treadmill training have been shown to promote walking and mobility measures.
Stretching can be helpful to prevent worsening of contractures (which are frequently seen in the CP population), however as a stand-alone treatment, they do not promote muscle length improvements, or improve function in those with CP. Further research is required to determine the most effective way to improve muscle length and function, however it appears that stretching alone is not an effective intervention.
Reference:
Kalkman BM, Bar-On L, O’Brien TD and Maganaris CN (2020) Stretching Interventions in Children With Cerebral Palsy: Why Are They Ineffective in Improving Muscle Function and How Can We Better Their Outcome? Front. Physiol. 11:131. doi: 10.3389/fphys.2020.00131